About the Cardinal Free Clinics
The Cardinal Free Clinics (CFCs) are two student run clinics located in the San Francisco Bay Area that are affiliated with the Stanford School of Medicine. The CFCs provide no-cost transitional primary and specialty care to a diverse demographic including patients that are low-income, uninsured, homeless, non-English speaking, or from otherwise disadvantaged populations. Arbor Free Clinic (Arbor) is located on the Veterans Affairs campus in Menlo Park, CA and has historically been open on Sundays from 8 am to 1 pm for walk-in patients. Pacific Free Clinic (PFC) is located in East San Jose, open on Saturdays from 8am-1pm for walk-in patients. You can find out more or donate to the clinics by clicking here.
Stanford Medicine Logo.


Summary
The CFCs are each managed by a group of four undergraduate and medical students and two medical directors. During my three years at the clinics, I had the honor of being a health educator, bridge to care counselor, quality improvement intern, and community outreach manager. I was able to significantly contribute to three quality improvement research projects aimed at improving care for the CFCs' patients. These projects consisted of developing a referrals tool, analyzing effectiveness of outreach activities, and reducing patient wait times.
Image by me.
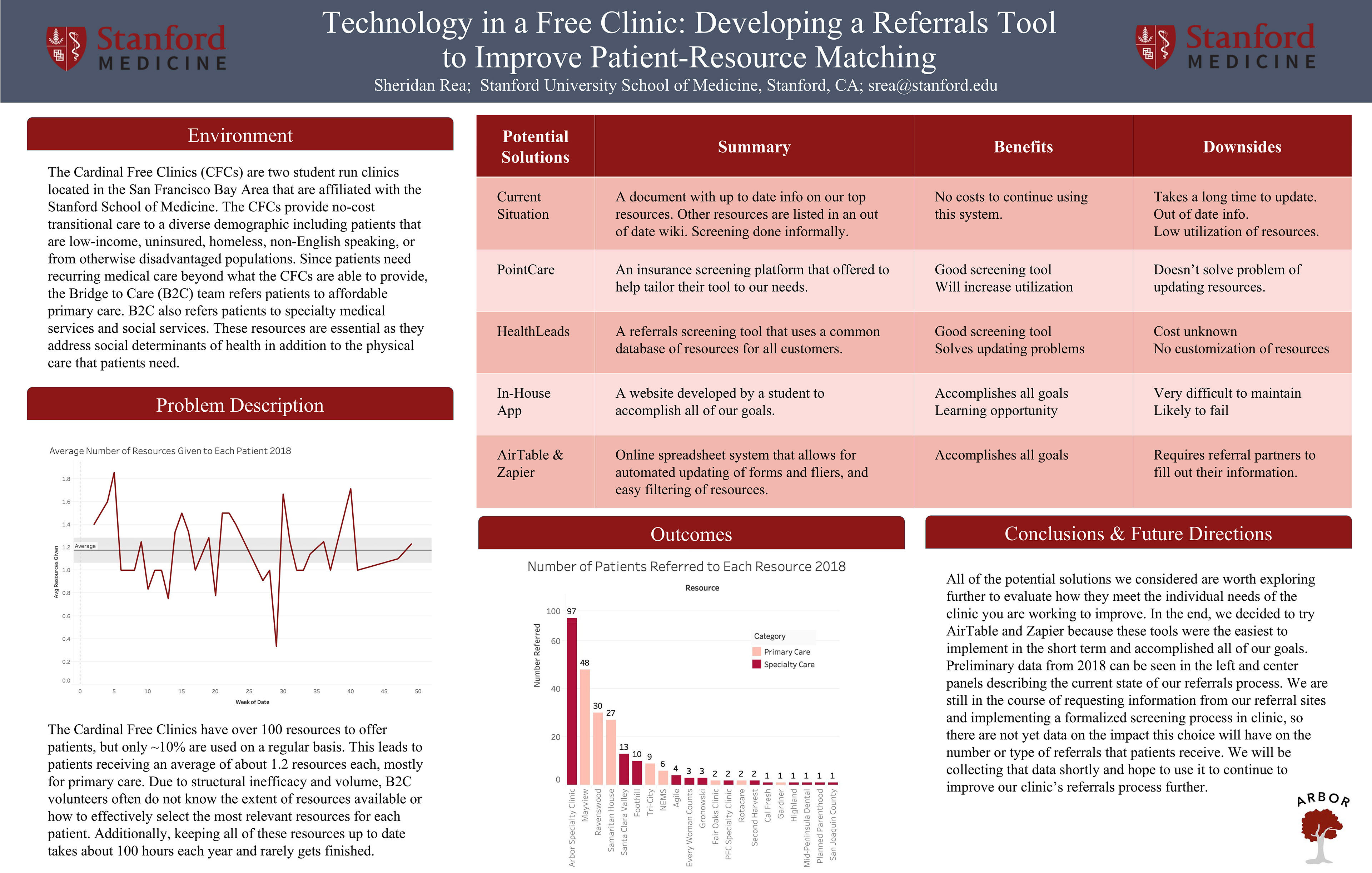
Technology in a Free Clinic:
Developing a New Referrals Tool to Improve Patient-Resource Matching
Team: Sheridan Rea, Tamara Montacute
Motivation
Patients seen at the CFCs frequently need recurring medical care beyond what the CFCs are able to provide. The Bridge to Care (B2C) team refers patients to affordable primary care. B2C also refers patients to specialty medical services and social services. These resources are essential as they address social determinants of health in addition to the physical care that patients need. The Cardinal Free Clinics have over 100 resources to offer patients, but only ~10% are used on a regular basis. Due to structural inefficacy and volume, B2C volunteers often do not know the extent of resources available or how to effectively select the most relevant resources for each patient. Accomplishing these tasks would require B2C volunteers to spend substantial time to gain the requisite familiarity and knowledge of the available resources and to keep that information up to date. I wanted to address this problem by creating a tool for our volunteers to use that would help them provide our patients with better resources.


Methods
Initially I came up with a solution to develop an in-house referrals screening tool from scratch. The CFC Screening Tool was going to be a database powered web application that would allow our volunteers to screen our patients in real time and provide them with the most relevant and up-to-date resources. The challenges of developing this tool in-house were compounded by the constraints of a resource-scarce environment, and ultimately I abandoned this approach when I realized it would be too difficult to maintain after I left the clinic. I considered other approaches such as using pre-existing services like PointCare and HealthLeads, but I found those options to either be too expensive (in time or money) or to lack the degree of customization I wanted for the CFCs. In the end I decided to combine AirTable, a spreadsheet-database hybrid, and Zapier, an automation tool, to create a database of resources that could be updated with a form sent out to our referrals partners or filled out by our volunteers and that could be filtered to easily obtain a list of resources best suited for an individual patient.
Image by Dirk Wouters from Pixabay.
Conclusions
The measurable outcomes this tool could affect are the number of referrals given, the number of successful referral connections, and the efficiency of the referrals team. In order to measure these outcomes tracking will be done on the number of referrals given and the efficiency of the referrals team through volunteer logging. Due to loss to follow up, tracking successful referrals is challenging with or without a screening tool, so this metric will not be measured. The efficiency of the referrals team will be measured by average number of hours spent in clinic standardized by the number of referrals given. This data has been collected prior to implementation of the tool, and the tool has been created, but data has not yet been collected post-implementation of the tool. I have since moved out of the area of the clinics and am no longer involved with this project, but I hope that this analysis is completed by my successors. While these results will not be generalizable to all student run clinics, the project may inspire students to consider how interdisciplinary collaborations with university departments outside of medicine as well as targeted operational improvements can be utilized to improve patient experience.
Poster presented at the Society of Student Run Free Clinics Conference in 2019.
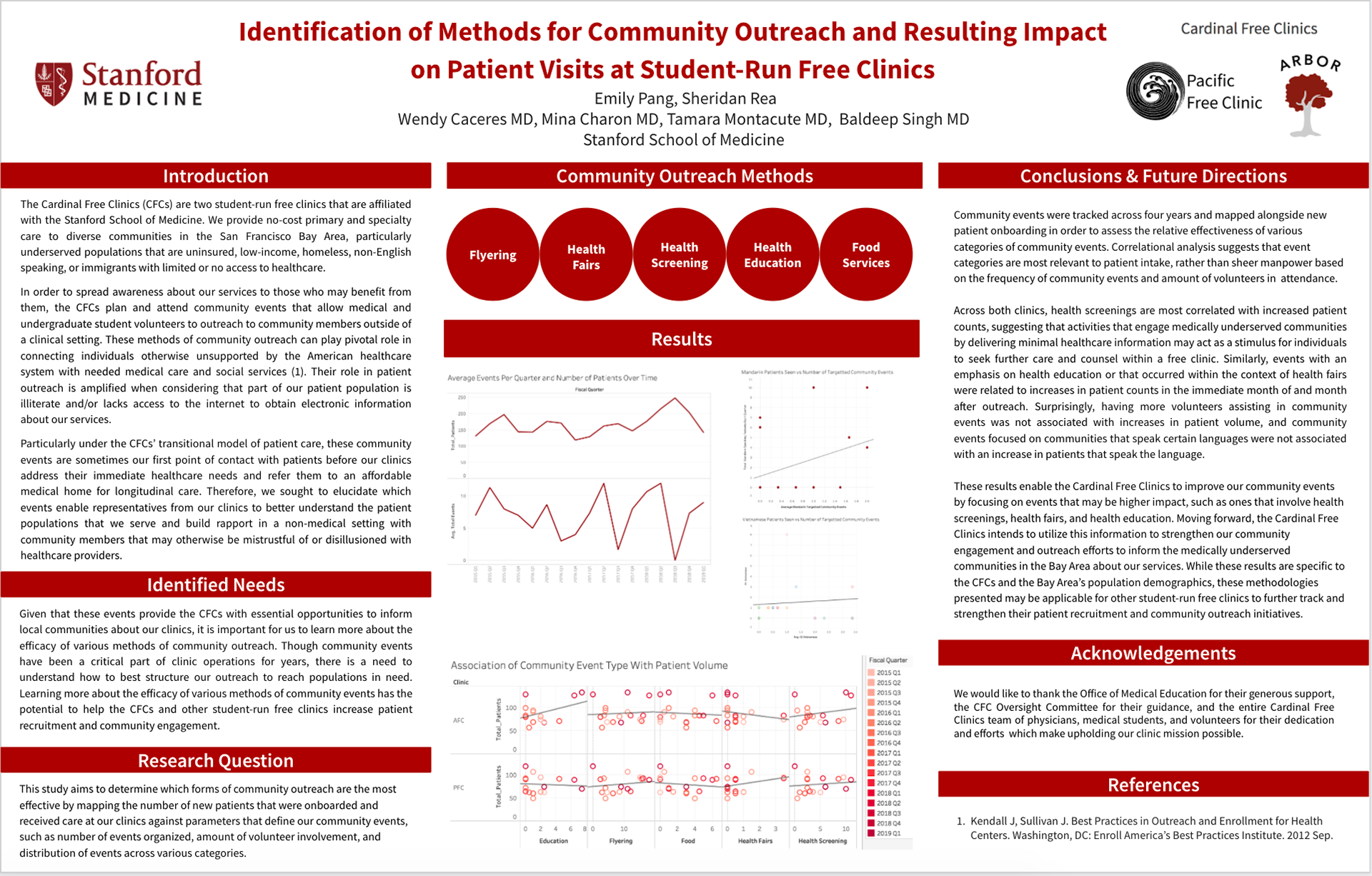
Identification of Methods for Community Outreach and Resulting Impact
on Patient Visits at Student-Run Free Clinics
Team: Emily Pang, Sheridan Rea, Wendy Caceres, Baldeep Singh
Motivation
In order to inform communities about our services, the CFCs plan and attend community events that allow medical and undergraduate student volunteers to interact with community members outside of a clinical setting. These events are extremely important for the CFCs because they provide us with essential opportunities to inform the community about our clinics; their role in patient outreach is amplified when considering that our patient population may lack access to the internet in order to obtain electronic information about the CFCs. These events also allow our volunteers to interact with community members in a non-medical setting and gain a better understanding of the patient population that we serve. Learning more about which community events are the most effective has the potential to help the CFCs and other student-run free clinics increase patient recruitment and community engagement.
Image by truthseeker08 from Pixabay.

Methods
This study aimed to determine which types of community events are the most effective by mapping the number of patients recruited to the categories of community events attended each year. Since new community event coordinators are recruited each year, there is clear grouping of community event strategy and type by year. Additionally there is variance by season, both in the type of community events planned and in patient numbers. We will controlled for potential differences due to confounding factors (such as K-12 school schedules and weather) by comparing community event strategies year to year in each season. Our null comparison group was an average of seasons during which no community events were planned or attended by clinic volunteers for the purpose of community engagement or patient recruitment.
Community events and descriptions are tracked every year in a spreadsheet and were categorized by students who have been attending events for several years. Examples of categories of community events are: health fairs, health screenings, flyering, food services, and educational programs. The number of new patients at each clinic during each season was pulled from the Point and Click EHR system used by the CFCs. Quantitative analyses were then conducted to determine which categories of events are most associated with higher patient turnout.
Image by Gerd Altmann from Pixabay.
Conclusion
Correlational analysis suggests that event categories, rather than sheer manpower, are most relevant to patient intake. Across both clinics, health screenings are the category most correlated with increased patient counts, suggesting that activities that engage medically underserved communities by delivering minimal healthcare information may act as a stimulus for individuals to seek further care at a free clinic. Similarly, events with an emphasis on health education or events that occurred within the context of health fairs were related to increases in patient counts in the immediate month of and month after outreach. Surprisingly, having more volunteers assisting in community events was not associated with increases in patient volume, and community events focused on communities that speak certain languages were not associated with an increase in patients that speak the language.
Moving forward, the Cardinal Free Clinics intends to utilize this information to strengthen our community engagement and outreach efforts to inform the medically underserved communities in the Bay Area about our services. While these results are specific to the CFCs and the Bay Area’s population demographics, the methodologies and results presented may be applicable for other student-run free clinics to strengthen their patient recruitment and community outreach initiatives.
Poster presented at the Society of Student Run Free Clinics Conference in 2019.
A Tale of Two Sister Clinics:
Comparing the Use of Online Scheduling Tools to Reduce Patient Wait Times
Team: Seul Ku, MS; Monica Liu; Sheridan Rea; Kabungo Mulumba; Annabel Chen; Ritika Dutta; Bina Kakusa; Wendy Caceres, MD; Baldeep Singh, MD; Mina Charon, MD; Tamara Montacute, MD
Motivation
Patients at the CFCs have traditionally been seen on a walk-in basis only, and on average, patients may wait more than an hour to be seen. Long waiting times are a somewhat notorious problem in healthcare delivery and have been shown to substantially decrease patient satisfaction (1,2). We quickly run into a problem because while queuing theory shows us that first come first serve systems have inherently longer wait times than those with appointments, not all of our patient population can easily access the internet to make appointments (3). Our operations managers came up with a compromise to have appointment slots scheduled throughout the clinic day, but to still see all walk-in patients. The idea being that by spreading out the appointments, some patients would be able to arrive later rather than waiting in line, thus hypothetically decreasing average wait time and increasing patient satisfaction. While the phenomenon of reduced waiting time due to the introduction of scheduled appointments has been studied extensively in various outpatient settings with staff available to schedule the appointments, it has not been studied in a student run free clinic using a self-serve online tool (3,6).
Image by S. Hermann & F. Richter from Pixabay.


Methods
At PFC, timepoints were recorded using the EHR, whereas the time points were manually collected by student managers at Arbor. Each time point was recorded on the patient intake sheet by an undergraduate or a medical student accompanying the patient throughout their visit. The following timepoints were collected: patient arrival in clinic, entrance of first healthcare provider into room, resident/attending entrance into room, patient departure from room, departure from clinic. This data was then transferred to Microsoft Excel. At Arbor, specialty clinic patients (dermatology, cardiology, ophthalmology, etc.) and follow-up visits were excluded given that the scheduling process is managed independently, whereas specialty clinic patients (women’s clinic, hepatology, dermatology, mental health and ophthalmology) at PFC were included. At both clinics, data points with missing arrival or ending times were also excluded.
Image by Robyn Wright from Pixabay.
Results and Conclusions
The total number of patients being seen on that day and whether or not patients had online appointments were significant determinants of wait times. Patients at Arbor with appointments had a median wait time of 35 min (n=46) compared to 60 min (n=232) without appointments (p<0.05). At PFC, patients with appointments waited 22 min (n=123) compared to 26 min (n=193) without appointments (p=0.08851). This data shows that a free online scheduling tool has the potential to significantly decrease patient wait times. Notably, the difference was much greater in one clinic; this is potentially due to differing management styles, student staff roles, and clinic flow.
This paper has been published here.
References
1. Bleustein C, Rothschild DB, Valen A, Valatis E, Schweitzer L, Jones R. Wait times, patient satisfaction scores, and the perception of care. Am J Manag Care. 2014;20(5):393-400. http://www.ncbi.nlm.nih.gov/pubmed/25181568. Accessed April 26, 2019.
2. JL Campbell. General Practitioner Appointment Systems, Patient Satisfaction, and use of Accident and Emergency Services—a Study in One Geographical Area. Fam Pract. 1994;11(4):438-445. doi:https://doi.org/10.1093/fampra/11.4.438
3. Fomundam SF, Herrmann JW. A Survey of Queuing Theory Applications in Healthcare.; 2007. https://drum.lib.umd.edu/bitstream/handle/1903/7222/tr_2007-24.pdf?sequence=1&isAllowed=y. Accessed April 26, 2019.
4. Ansell D, Crispo JAG, Simard B, Bjerre LM. Interventions to reduce wait times for primary care appointments: a systematic review. BMC Health Serv Res. 2017;17(1):295. doi:10.1186/s12913-017-2219-y
5. Silvester K, Lendon R, Bevan H, Steyn R, Walley P. Reducing waiting times in the NHS: Is lack of capacity the problem? | Request PDF. Clin Manag. 2004;12(3):105-111. https://www.researchgate.net/publication/233662085_Reducing_waiting_times_in_the_NHS_Is_lack_of_capacity_the_problem. Accessed May 9, 2019.
6. Eilers GM. Improving Patient Satisfaction With Waiting Time. J Am Coll Heal. 2004;53(1):41-48. doi:10.3200/JACH.53.1.41-48
7. Lu, K. B., Thiel, B., Atkins, C. A., Desai, A., Botwin, A., Povlow, M. R., … Pasarica, M. (n.d.). Satisfaction with Healthcare Received at an Interprofessional Student-run Free Clinic: Invested in Training the Next Generation of Healthcare Professionals. Cureus, 10(3). https://doi.org/10.7759/cureus.2282

Sheridan Rea

Seul Ku

Monica Liu

Kabungo Mulumba
Annabel Chen

Emily Pang

Ritika Dutta

Bina Kakusa
Dr. Wendy Caceres

Dr. Baldeep Singh

Dr. Mina Charon
