Summary
The Virtual Hypertension Management project (VHM) aims to evaluate the effectiveness of using bluetooth-enabled EHR-connected blood pressure cuffs to manage hypertension. Our hypothesis is that through greater access to BP data patients will experience higher self-efficacy to change behaviours and providers will be able to titrate medications more rapidly in order to bring BP under control. I helped define study endpoints, wrote the patient survey, presented a poster at AMIA, conducted the data analysis, and will assist with writing the manuscript. This research will likely be submitted for publication in 2020.
Image by Myriam Zilles from Pixabay.

Motivation
Hypertension is second only to tobacco use as a leading cause of preventable death (1). With just over 50% of Americans with hypertension at goal pressures, a 10% increase in management would save an estimated 14,000 lives per year (2). The current clinical model, despite being informed by adequate knowledge of effective treatment, falls short of managing hypertension for several reasons (3,4). First, in addition to possible misdiagnoses due to white coat hypertension, intermittent blood pressure (BP) monitoring in clinic can lead to a major risk of adverse events due to low BP outside of clinic. Second, the in-person practice to establish a diagnosis and achieve target pressures places an undue burden on both the patient and the health care system and significantly contributes to patients lost to follow-up and resultant missed opportunity to achieve target pressures. Home hypertension monitoring and management has proven an effective option to improve clinical outcomes and increase patient and provider experience (5). However, challenges integrating patient-collected data into clinician workflow has limited widespread adoption even with national leaders in healthcare quality improvement such as Kaiser Permanente. This project aims to examine the clinical outcomes and usability of a virtual management model using home BP cuffs that integrate with patients’ smart phone and electronic medical records. Integrating home data into clinicians’ usual workflow, via the electronic health record (EHR) may lead to increased patient engagement, provider efficiency, and lower resource utilization.
Image by Ernesto Eslava from Pixabay.
Methods
We recruited uncontrolled hypertensive patients from Stanford primary care clinics in Santa Clara and Palo Alto. Eligible patients are randomly assigned 1:1 to either usual care, consisting of pharmacist-led hypertension management, or usual care plus the ability to transmit home BP data, automatically, to our EHR. Both groups received an identical BP cuff. The timing and frequency of BP measurements was directed by the pharmacist as per usual care, and we did not provide extra reminders outside of this. We will be able to see the time of the measurements in the EHR.
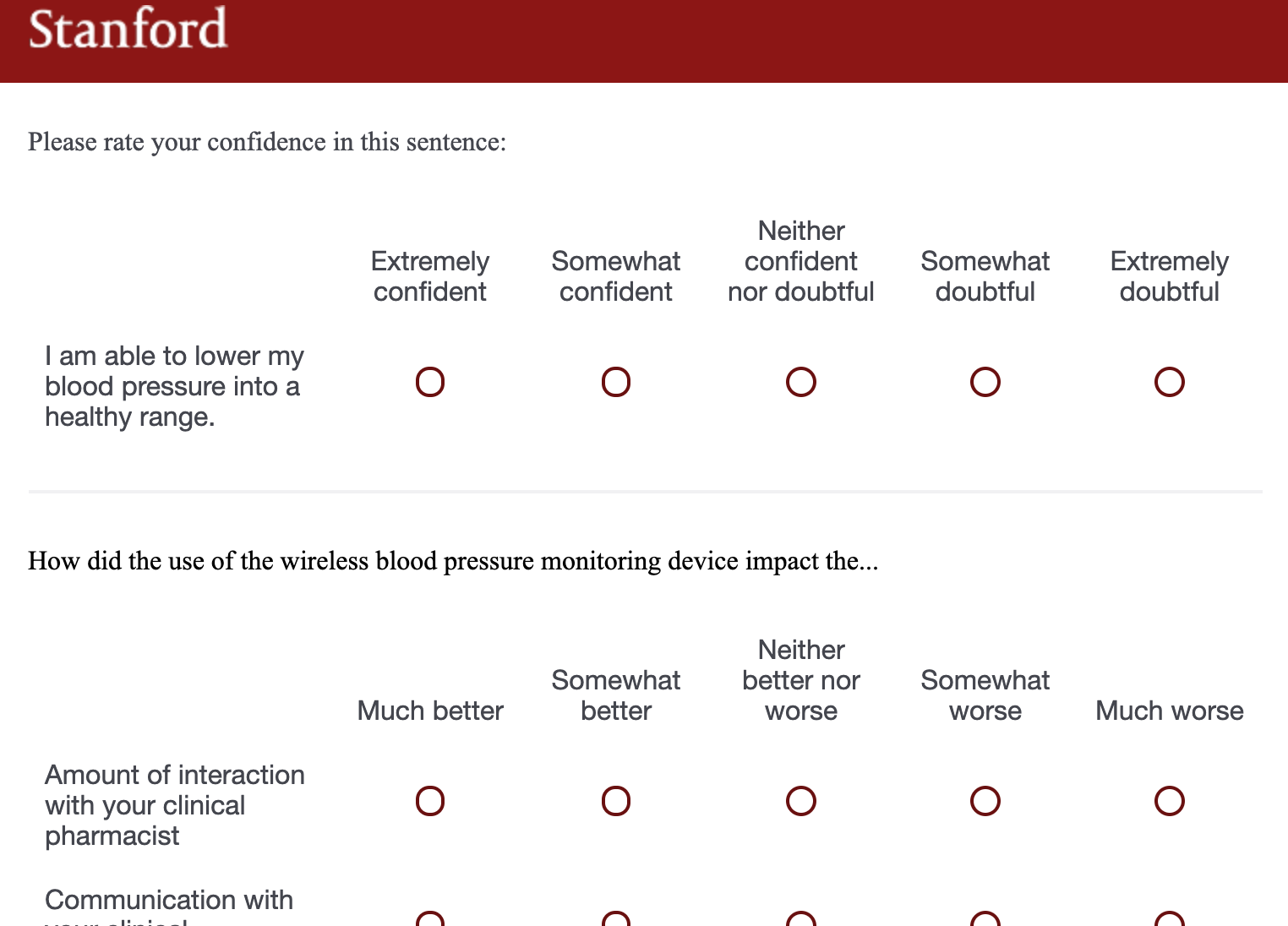
The primary outcome is the change in BP of patients over a 6-month period in the control group vs the intervention group. Secondary outcomes include frequency of patient visits to clinic, patient remote interactions, number of medication changes, and time to reach BP control. We will also be examining patient and provider satisfaction with using a connected device and investigating barriers to use.
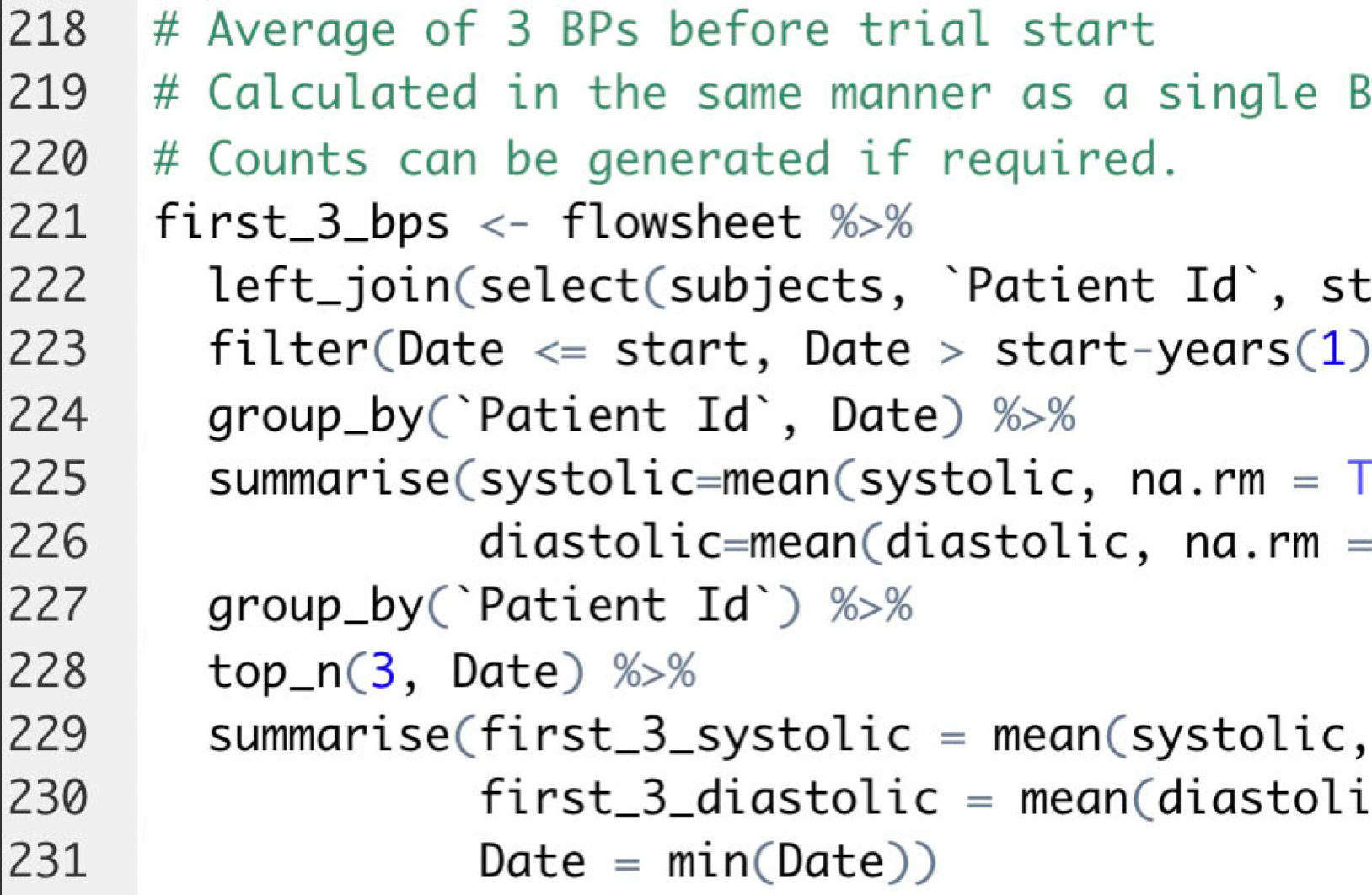
Images by me.
Expected Results and Future Directions
We anticipate that using a connected BP cuff integrated with the patient’s electronic medical record will be acceptable and preferable to usual care to both patients and providers and potentially allow clinicians to titrate medications faster and with fewer clinic visits. This may lead to greater decreases in BP or faster times to controlled BP. Qualitative analysis of patient and provider satisfaction will likely provide information on barriers to use and how this technology can be better optimized to achieve higher usage rates and greater reductions in BPs.
Possible avenues of future inquiry include algorithm based titration, video conference appointments, and targeting special populations for whom close BP monitoring is important, such as patients who are post-stroke, peripartum, or have chronic kidney disease. This information may be valuable to health systems seeking to deploy EHR-connected devices in new clinical care delivery models.
I chose to work on this project because I wanted to learn about clinical research practices, work with patients instead of with lab samples, and apply technology advancements to medicine. Medicine has been on the forefront of technological innovation in a small number of cases, but systematically falls behind in the adoption of technology used widely in other industries. Hypertension is particularly interesting to me because we know how to treat it effectively yet still see so many patients failing to achieve BP control. I expect that truly addressing this problem will require changing society rather than just medicine (i.e. safer neighborhoods, more paid time off, healthier eating culture, transparent universal insurance), but I have enjoyed using my statistical and research knowledge to determine if outcomes can be improved with the remote management of hypertension. This project has sparked my long-term interest in health services and outcomes research.
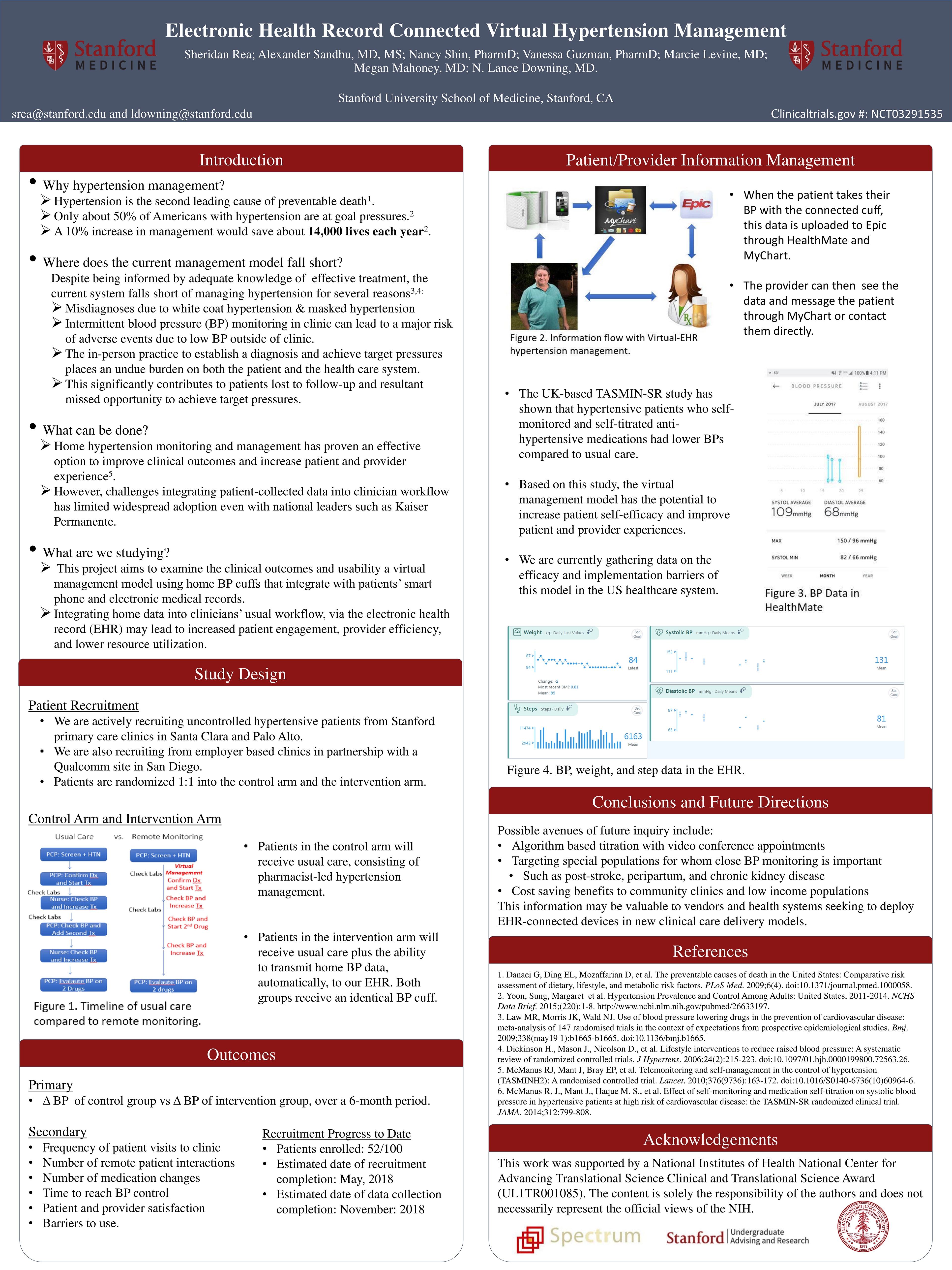
Poster presented at the American Medical Informatics Association's 2018 Informatics Summit.

Sheridan Rea

Dr. Alexander Sandhu
Dr. Nancy Shin

Dr. Vanessa Guzman

Dr. Marcie Levine

Dr. Megan Mahoney

Dr. Lance Downing
References
1. Danaei G, Ding EL, Mozaffarian D, et al. The preventable causes of death in the United States: Comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med. 2009;6(4). doi:10.1371/journal.pmed.1000058.
2. Yoon, Sung, Margaret et al. Hypertension Prevalence and Control Among Adults: United States, 2011-2014. NCHS Data Brief. 2015;(220):1-8. http://www.ncbi.nlm.nih.gov/pubmed/26633197.
3. Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. Bmj. 2009;338(may19 1):b1665-b1665. doi:10.1136/bmj.b1665.
4. Dickinson H., Mason J., Nicolson D., et al. Lifestyle interventions to reduce raised blood pressure: A systematic review of randomized controlled trials. J Hypertens. 2006;24(2):215-223. doi:10.1097/01.hjh.0000199800.72563.26.
5. McManus RJ, Mant J, Bray EP, et al. Telemonitoring and self-management in the control of hypertension (TASMINH2): A randomised controlled trial. Lancet. 2010;376(9736):163-172. doi:10.1016/S0140-6736(10)60964-6.